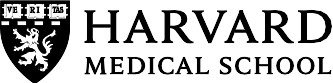

Understand what your heart cardiovascular testing results really mean
See your biomarkers in context with a comprehensive panel.
- CLIA-certified labs
- HIPAA compliant
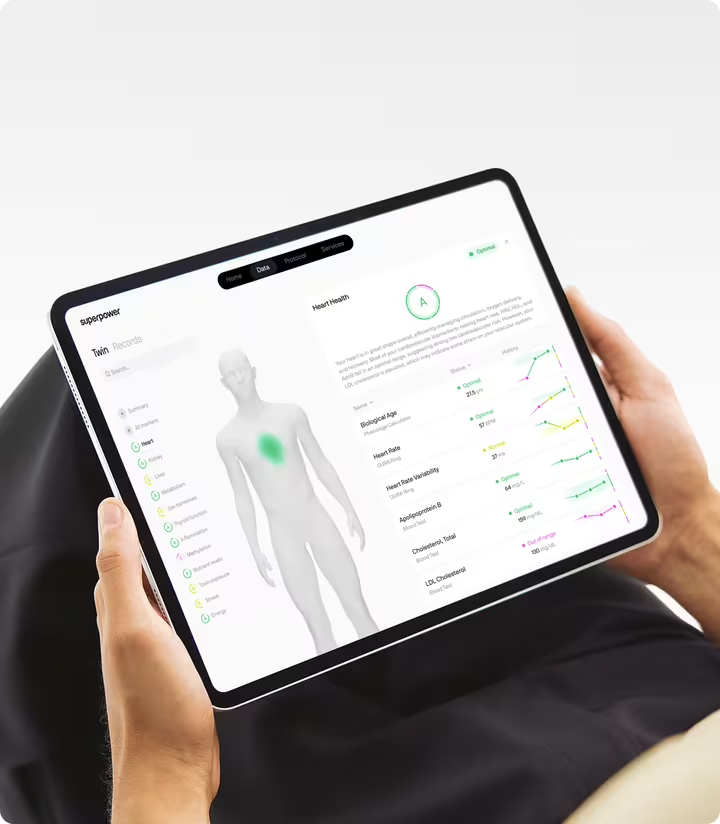
- Personalized health protocol
Lipoprotein(a), defined as an inherited cholesterol particle
Lipoprotein(a) is a cholesterol-carrying particle made in the liver — an LDL particle with an extra protein, apolipoprotein(a), covalently linked to its apoB-100 backbone. That structural addition changes the biology in ways that matter for arteries and heart valves, independently raising risk for atherosclerotic cardiovascular disease and calcific aortic valve stenosis. Units can be confusing: labs report Lp(a) in mg/dL or nmol/L, but because particle size varies by apo(a) isoform, the two units are not interchangeable with a single conversion factor. Modern, isoform-insensitive assays reporting in nmol/L are preferred. No fasting is required.
Why lp(a) is largely written by your genes
Lp(a) works through two overlapping mechanisms. First, it carries cholesterol and oxidized phospholipids directly into the artery wall, fueling plaque growth and local inflammation. Second, its apo(a) component structurally resembles plasminogen — a key clot-dissolving protein — and can interfere with fibrinolysis, tilting the system toward thrombosis when plaques rupture. In heart valves, Lp(a) drives microscopic calcification that can, over years, stiffen the aortic valve.
Approximately 80 to 90 percent of your Lp(a) level is determined by the LPA gene, making it one of the most genetically anchored biomarkers in cardiovascular medicine. Decades of Mendelian randomization studies and prospective cohorts confirm that higher Lp(a) independently raises the risk of heart attacks, atherosclerotic stroke, and calcific aortic valve disease — on top of LDL cholesterol and other conventional risk factors. Because the level is genetically set and stable across adult life, a single well-measured value carries meaningful lifetime information. It does not respond meaningfully to diet or standard lifestyle changes — a key distinction from most other lipid markers.
What your lp(a) number actually means
Reference ranges and thresholds
Lab reference intervals describe the middle of a population, not a promise of health. With Lp(a), what matters is predictive risk, not what is common. Many professional societies use the following practical cut points: below approximately 75 nmol/L (roughly below 30 mg/dL) is generally considered low risk; 75 to 125 nmol/L (about 30 to 50 mg/dL) is intermediate; above 125 nmol/L (greater than 50 mg/dL) is high, with risk rising as the number climbs. Because different labs use different assays, always interpret your result in the context of the units and method used — mg/dL and nmol/L values are not interchangeable.
Levels differ by ancestry and life stage. People of African ancestry tend to have higher average Lp(a). Levels can increase after menopause. Children generally resemble their adult pattern by late childhood. "Optimal" is therefore personal and contextual — the goal is to calibrate your risk conversation, not to assign a label.
When levels run high
If your Lp(a) is elevated, the most likely explanation is genetics. That is not a diagnosis or a destiny — it means your arteries may be exposed to more pro-atherogenic, pro-inflammatory particles over time. The signal strengthens when high Lp(a) travels alongside high apoB, elevated LDL cholesterol, high blood pressure, or a family history of early heart disease.
Secondary elevations also occur: chronic kidney disease can raise Lp(a), levels climb during pregnancy and usually return toward baseline postpartum, and menopause can coincide with higher values. Acute illness can nudge levels transiently, so if a result seems out of character, repeating the test when you are well is reasonable. A persistent elevation across repeat tests in a steady state carries the most weight. For guidance on what a confirmed elevated result means for management, see symptoms of high lipoprotein(a).
When levels run low
Low Lp(a) is common and generally favorable for cardiovascular risk, usually reflecting genetics and occasionally hormone effects. Estrogen therapy can lower Lp(a) in postmenopausal women, though it is not used solely for that purpose. Some genetic studies hint at a modest association between extremely low Lp(a) and higher type 2 diabetes risk, but clinical implications are unclear and not used to guide care. In practice, low Lp(a) simply means one less source of arterial friction.
What lp(a) responds to, and what it doesn't
Because Lp(a) is so strongly genetically determined, most of the levers that move other lipid markers do not move it. Diet does not meaningfully shift Lp(a). Exercise does not shift it. Statins — foundational for lowering LDL cholesterol and apoB — do not lower Lp(a) and may nudge it slightly upward.
A smaller set of interventions does affect it. PCSK9 inhibitors lower Lp(a) by approximately 20 to 30 percent, with cardiovascular outcome benefits largely driven by their larger apoB reductions. Niacin lowers Lp(a) by approximately 20 to 30 percent but did not show added cardiovascular benefit in outcomes trials and carries a significant side-effect burden, so it is not routinely recommended. For very high Lp(a) with progressive disease, lipoprotein apheresis can acutely reduce levels and is used selectively at specialized centers. Investigational siRNA therapies — including pelacarsen and olpasiran — have shown reductions of 80 to 90 percent in trials, with large outcomes studies ongoing.
Secondary factors that can elevate Lp(a) include chronic kidney disease, pregnancy, menopause, and acute illness. Assay method matters: nmol/L is preferred over mg/dL for comparability across labs.
Reading lp(a) alongside the standard lipid panel
- Apolipoprotein B (ApoB) — each Lp(a) particle carries one ApoB molecule, so high Lp(a) inflates total ApoB above what LDL particle count alone would predict. ApoB contextualizes whether the overall atherogenic particle burden is driven by Lp(a), LDL, or both.
- LDL cholesterol — Lp(a)'s cholesterol content is counted within calculated LDL-C by the Friedewald equation. A discordance between LDL-C and ApoB in someone with high Lp(a) may partly reflect this inflation, making ApoB the more reliable particle-burden metric in this context.
- High-sensitivity CRP (hs-CRP) — Lp(a) carries oxidized phospholipids that drive vascular inflammation. hs-CRP reveals whether arterial inflammation is currently active alongside the genetic risk signal, helping distinguish a quiet elevated Lp(a) from one operating in an already-inflamed environment.
- Non-HDL cholesterol — non-HDL cholesterol captures all ApoB-containing cholesterol, including Lp(a)-associated cholesterol. It is a practical, widely available surrogate for total atherogenic cholesterol burden when a full particle panel is not available.
- Symptoms of high lipoprotein(a) — the management and symptom-context article for elevated Lp(a). Readers with a confirmed high result can follow here for actionable guidance on what the elevation means in practice.

Test 100+ biomarkers from home
One blood draw. A full picture of your health, explained in plain language.
Test 100+ biomarkers from home
One blood draw. A full picture of your health, explained in plain language.
Why lp(a) is a one-time measurement for most people
Approximately 80 to 90 percent of your Lp(a) level is determined by the LPA gene — it is one of the most genetically anchored biomarkers in cardiovascular medicine. Lp(a) does not respond to diet, exercise, or statin therapy in any clinically significant way. Your Lp(a) level is unlikely to change much. A single accurate measurement is usually enough. Recheck only if your therapy or your underlying condition changes.
Recheck is warranted if you start a therapy known to affect Lp(a) — such as a PCSK9 inhibitor or an investigational siRNA agent — if you develop chronic kidney disease or hypothyroidism, or if you need to confirm the result because the initial assay was reported in mg/dL and an nmol/L comparison is needed for clinical decision-making. Do not apply the 8-to-12-week retest cadence used for responsive markers like LDL cholesterol or triglycerides. Some numbers are designed to be measured once. This is one of them.
When an lp(a) result reshapes your prevention plan
A once-in-a-lifetime Lp(a) test can explain family patterns, sharpen your lifetime risk estimate, and steer earlier course corrections. If your result is elevated, the most evidence-based response is to drive down total apoB, control blood pressure, and treat the whole risk profile — because those are the levers that do move. Some guidelines suggest low-dose aspirin may offer added protection in people with high Lp(a) and low bleeding risk; that is a personalized discussion with your clinician. Coronary artery calcium imaging can help determine whether genetic risk has already translated into measurable plaque.
Most of the time, Lp(a) serves as a steady reference point while you work the modifiable factors: apoB, blood pressure, glucose control, fitness, and inflammation. Data is most powerful when it matches how you feel and function — trend your results alongside your clinical picture, and let the pattern guide smarter next steps. For readers who want to understand what a confirmed elevated result means for symptoms and management, symptoms of high lipoprotein(a) covers that ground in full.
When you see Lp(a) next to apoB, LDL cholesterol, non-HDL cholesterol, and inflammation markers, the pattern becomes clear. You move from generic targets to a plan that matches your biology, with room to adapt as new therapies arrive. That is the promise of a comprehensive panel done well: fewer blind spots, better timing, and decisions made with confidence and calm in partnership with a clinician. Superpower is built around that approach — you can read more about it at our manifesto.
Frequently Asked Questions
References
- Kronenberg F, Mora S, Stroes ESG, Ference BA, Arsenault BJ, Berglund L, Dweck MR, Koschinsky M, Lambert G, Mach F, McNeal CJ, Moriarty PM, Natarajan P, Nordestgaard BG, Parhofer KG, Virani SS, von Eckardstein A, Watts GF, Stock JK, ... Catapano AL (2022). Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. *European heart journal*, *43*(39), 3925-3946. https://doi.org/10.1093/eurheartj/ehac361
- Reyes-Soffer G, Ginsberg HN, Berglund L, Duell PB, Heffron SP, Kamstrup PR, Lloyd-Jones DM, Marcovina SM, Yeang C, Koschinsky ML, American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; and Council on Peripheral Vascular Disease (2022). Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. *Arteriosclerosis, thrombosis, and vascular biology*, *42*(1), e48-e60. https://doi.org/10.1161/ATV.0000000000000147
- Burgess S, Ference BA, Staley JR, Freitag DF, Mason AM, Nielsen SF, Willeit P, Young R, Surendran P, Karthikeyan S, Bolton TR, Peters JE, Kamstrup PR, Tybjærg-Hansen A, Benn M, Langsted A, Schnohr P, Vedel-Krogh S, Kobylecki CJ, ... Danesh J, European Prospective Investigation Into Cancer and Nutrition–Cardiovascular Disease (EPIC-CVD) Consortium (2018). Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. *JAMA cardiology*, *3*(7), 619-627. https://doi.org/10.1001/jamacardio.2018.1470
- Thanassoulis G, Campbell CY, Owens DS, Smith JG, Smith AV, Peloso GM, Kerr KF, Pechlivanis S, Budoff MJ, Harris TB, Malhotra R, O'Brien KD, Kamstrup PR, Nordestgaard BG, Tybjaerg-Hansen A, Allison MA, Aspelund T, Criqui MH, Heckbert SR, ... Post WS, CHARGE Extracoronary Calcium Working Group (2013). Genetic associations with valvular calcification and aortic stenosis. *The New England journal of medicine*, *368*(6), 503-12. https://doi.org/10.1056/NEJMoa1109034
- O'Donoghue ML, Rosenson RS, Gencer B, López JAG, Lepor NE, Baum SJ, Stout E, Gaudet D, Knusel B, Kuder JF, Ran X, Murphy SA, Wang H, Wu Y, Kassahun H, Sabatine MS, OCEAN(a)-DOSE Trial Investigators (2022). Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease. *The New England journal of medicine*, *387*(20), 1855-1864. https://doi.org/10.1056/NEJMoa2211023
- O'Donoghue ML, Fazio S, Giugliano RP, Stroes ESG, Kanevsky E, Gouni-Berthold I, Im K, Lira Pineda A, Wasserman SM, Češka R, Ezhov MV, Jukema JW, Jensen HK, Tokgözoğlu SL, Mach F, Huber K, Sever PS, Keech AC, Pedersen TR, Sabatine MS (2019). Lipoprotein(a), PCSK9 Inhibition, and Cardiovascular Risk. *Circulation*, *139*(12), 1483-1492. https://doi.org/10.1161/CIRCULATIONAHA.118.037184