Diagnostic Test
Grail Galleri Multi Cancer Test
$999
+ membership
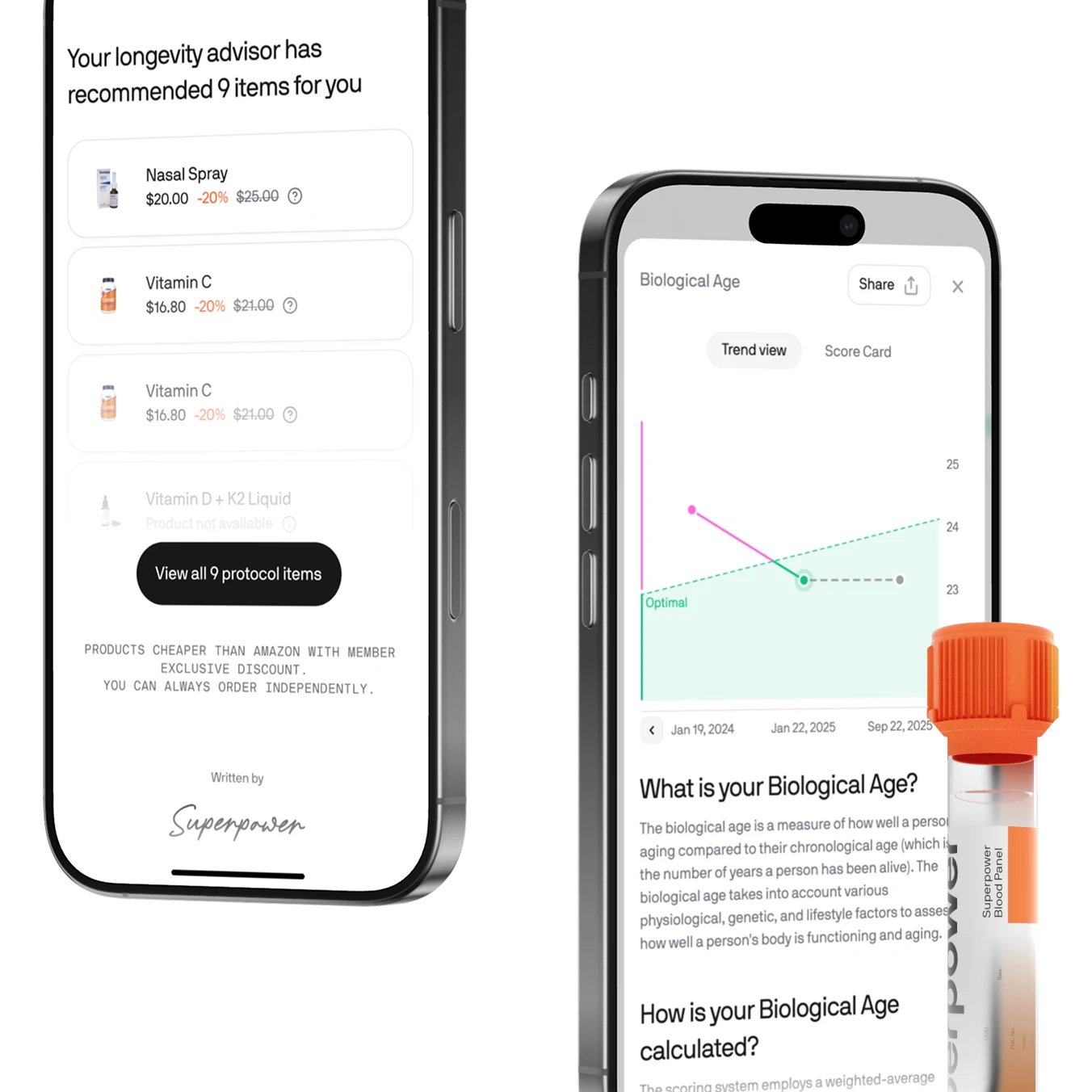
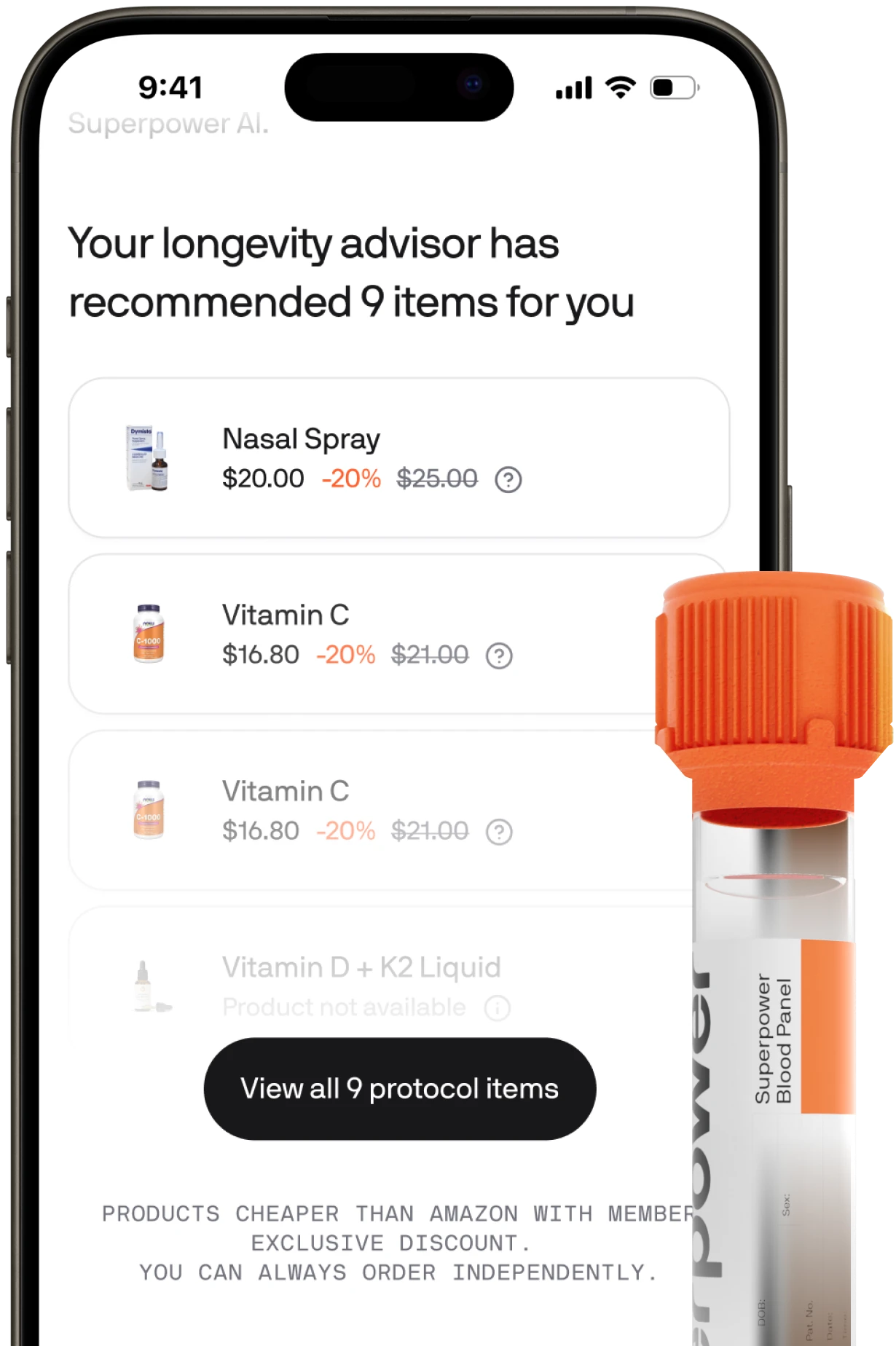
Screen for 50+ cancer types with one blood test. Advanced DNA sequencing and machine learning detect early cancer signals before symptoms appear, enabling proactive treatment when outcomes are best.
Early detection: Screen for 50+ cancer types from a single blood test
Advanced technology: Analyzes over 1 million DNA sites using machine learning
Convenient at-home testing: Licensed phlebotomist visit, no fasting required
Fast results: Receive comprehensive results in 2-3 weeks via your dashboard
HSA / FSA Eligible
At-lab/At-home testing

'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3crect%20x='2'%20y='1.25'%20width='39'%20height='23'%20rx='5.5'%20stroke='%2309090B'%20stroke-opacity='0.1'/%3e%3cpath%20d='M26.1103%207.81335C23.9472%207.81335%2022.0142%208.93483%2022.0142%2011.0068C22.0142%2013.383%2025.4425%2013.5471%2025.4425%2014.7408C25.4425%2015.2435%2024.8666%2015.6934%2023.8831%2015.6934C22.4873%2015.6934%2021.444%2015.0647%2021.444%2015.0647L20.9977%2017.1555C20.9977%2017.1555%2022.1995%2017.6866%2023.795%2017.6866C26.1599%2017.6866%2028.0209%2016.5101%2028.0209%2014.4027C28.0209%2011.8918%2024.5783%2011.7326%2024.5783%2010.6246C24.5783%2010.2308%2025.051%209.79945%2026.0317%209.79945C27.1383%209.79945%2028.0411%2010.2567%2028.0411%2010.2567L28.478%208.23724C28.478%208.23724%2027.4956%207.81335%2026.1103%207.81335ZM6.32044%207.96575L6.26807%208.27055C6.26807%208.27055%207.17807%208.43716%207.99766%208.76947C9.05298%209.15054%209.12815%209.37239%209.3059%2010.0614L11.2426%2017.5294H13.8388L17.8384%207.96575H15.2482L12.6782%2014.4682L11.6295%208.95643C11.5333%208.32561%2011.0461%207.96575%2010.4498%207.96575H6.32044ZM18.88%207.96575L16.848%2017.5294H19.3181L21.3429%207.96575H18.88ZM32.6561%207.96575C32.0605%207.96575%2031.7449%208.28471%2031.5134%208.84209L27.8947%2017.5294H30.4849L30.9861%2016.0815H34.1417L34.4464%2017.5294H36.7319L34.7381%207.96575H32.6561ZM32.993%2010.5495L33.7608%2014.1383H31.7038L32.993%2010.5495Z'%20fill='%231434CB'/%3e%3c/g%3e%3cdefs%3e%3cfilter%20id='filter0_d_50_1350'%20x='0'%20y='0'%20width='43'%20height='27'%20filterUnits='userSpaceOnUse'%20color-interpolation-filters='sRGB'%3e%3cfeFlood%20flood-opacity='0'%20result='BackgroundImageFix'/%3e%3cfeColorMatrix%20in='SourceAlpha'%20type='matrix'%20values='0%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%20127%200'%20result='hardAlpha'/%3e%3cfeOffset%20dy='0.75'/%3e%3cfeGaussianBlur%20stdDeviation='0.75'/%3e%3cfeComposite%20in2='hardAlpha'%20operator='out'/%3e%3cfeColorMatrix%20type='matrix'%20values='0%200%200%200%200.894118%200%200%200%200%200.894118%200%200%200%200%200.905882%200%200%200%200.5%200'/%3e%3cfeBlend%20mode='normal'%20in2='BackgroundImageFix'%20result='effect1_dropShadow_50_1350'/%3e%3cfeBlend%20mode='normal'%20in='SourceGraphic'%20in2='effect1_dropShadow_50_1350'%20result='shape'/%3e%3c/filter%3e%3c/defs%3e%3c/svg%3e)
'%3e%3cg%20clip-path='url(%23clip0_50_1352)'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='%23006FCF'/%3e%3cg%20clip-path='url(%23clip1_50_1352)'%3e%3cpath%20d='M41%200.750244H17V24.7502H41V0.750244Z'%20fill='white'/%3e%3cpath%20d='M17%200.750244V24.7502H41V20.9582H37.688L36.464%2019.5264L35.192%2020.9582H25.784V13.3344H22.6798L26.5602%204.5504H30.3358L31.2478%206.5424V4.5504H35.936L36.7198%206.6384L37.4878%204.5504H41V0.750244H17ZM38.288%205.79024L37.0558%209.0384L36.728%209.91872L36.392%209.0384L35.1522%205.79024H32.4402V12.1906H34.0722V8.02272L34.064%207.18224L34.3842%208.02272L35.9442%2012.1906H37.496L39.0642%208.02272L39.368%207.1904V12.1906H41V5.79024H38.288ZM27.44%205.79024L24.608%2012.1906H26.4637L26.96%2010.9584H30.0642L30.56%2012.1906H32.4402L29.624%205.79024H27.44ZM28.1917%207.9584L28.5118%207.15872L28.832%207.9584L29.4958%209.57408H27.5278L28.1917%207.9584ZM38.4162%2013.3426L36.488%2015.4142L34.568%2013.3426H32.4402H27.0958V19.7184H32.4402V18.3346H28.7278V17.2224H32.3682V15.8467H28.7278V14.7264H32.4402V13.3426L35.4238%2016.5422L32.4402%2019.7184H34.5042L36.4482%2017.6386L38.384%2019.7184H40.5037L37.5118%2016.5182L40.5037%2013.3426H38.4162ZM39.1918%2016.5106L41%2018.3504V14.6942L39.1918%2016.5106Z'%20fill='%23006FCF'/%3e%3c/g%3e%3c/g%3e%3crect%20x='2'%20y='1.25'%20width='39'%20height='23'%20rx='5.5'%20stroke='%2309090B'%20stroke-opacity='0.1'/%3e%3c/g%3e%3cdefs%3e%3cfilter%20id='filter0_d_50_1352'%20x='0'%20y='0'%20width='43'%20height='27'%20filterUnits='userSpaceOnUse'%20color-interpolation-filters='sRGB'%3e%3cfeFlood%20flood-opacity='0'%20result='BackgroundImageFix'/%3e%3cfeColorMatrix%20in='SourceAlpha'%20type='matrix'%20values='0%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%20127%200'%20result='hardAlpha'/%3e%3cfeOffset%20dy='0.75'/%3e%3cfeGaussianBlur%20stdDeviation='0.75'/%3e%3cfeComposite%20in2='hardAlpha'%20operator='out'/%3e%3cfeColorMatrix%20type='matrix'%20values='0%200%200%200%200.894118%200%200%200%200%200.894118%200%200%200%200%200.905882%200%200%200%200.5%200'/%3e%3cfeBlend%20mode='normal'%20in2='BackgroundImageFix'%20result='effect1_dropShadow_50_1352'/%3e%3cfeBlend%20mode='normal'%20in='SourceGraphic'%20in2='effect1_dropShadow_50_1352'%20result='shape'/%3e%3c/filter%3e%3cclipPath%20id='clip0_50_1352'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3c/clipPath%3e%3cclipPath%20id='clip1_50_1352'%3e%3crect%20width='24'%20height='24'%20fill='white'%20transform='translate(17%200.75)'/%3e%3c/clipPath%3e%3c/defs%3e%3c/svg%3e)
'%3e%3cg%20clip-path='url(%23clip0_50_1357)'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='%2318181B'/%3e%3crect%20width='39.9999'%20height='25.641'%20transform='translate(1.5%20-0.0704956)'%20fill='white'/%3e%3cpath%20d='M24.5415%207.2699H18.4409V18.2302H24.5415V7.2699Z'%20fill='%23FF5A00'/%3e%3cpath%20d='M18.8465%2012.75C18.8465%2010.5232%2019.8933%208.54682%2021.4997%207.26985C20.3175%206.34034%2018.8261%205.77856%2017.1995%205.77856C13.346%205.77856%2010.228%208.89653%2010.228%2012.75C10.228%2016.6035%2013.346%2019.7215%2017.1995%2019.7215C18.8261%2019.7215%2020.3175%2019.1597%2021.4997%2018.2302C19.8911%2016.9712%2018.8465%2014.9768%2018.8465%2012.75Z'%20fill='%23EB001B'/%3e%3cpath%20d='M32.7716%2012.75C32.7716%2016.6035%2029.6536%2019.7215%2025.8002%2019.7215C24.1735%2019.7215%2022.6822%2019.1597%2021.5%2018.2302C23.1267%2016.951%2024.1532%2014.9768%2024.1532%2012.75C24.1532%2010.5232%2023.1064%208.54682%2021.5%207.26985C22.68%206.34034%2024.1713%205.77856%2025.7979%205.77856C29.6536%205.77856%2032.7716%208.91685%2032.7716%2012.75Z'%20fill='%23F79E1B'/%3e%3c/g%3e%3crect%20x='2'%20y='1.25'%20width='39'%20height='23'%20rx='5.5'%20stroke='%2309090B'%20stroke-opacity='0.1'/%3e%3c/g%3e%3cdefs%3e%3cfilter%20id='filter0_d_50_1357'%20x='0'%20y='0'%20width='43'%20height='27'%20filterUnits='userSpaceOnUse'%20color-interpolation-filters='sRGB'%3e%3cfeFlood%20flood-opacity='0'%20result='BackgroundImageFix'/%3e%3cfeColorMatrix%20in='SourceAlpha'%20type='matrix'%20values='0%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%20127%200'%20result='hardAlpha'/%3e%3cfeOffset%20dy='0.75'/%3e%3cfeGaussianBlur%20stdDeviation='0.75'/%3e%3cfeComposite%20in2='hardAlpha'%20operator='out'/%3e%3cfeColorMatrix%20type='matrix'%20values='0%200%200%200%200.894118%200%200%200%200%200.894118%200%200%200%200%200.905882%200%200%200%200.5%200'/%3e%3cfeBlend%20mode='normal'%20in2='BackgroundImageFix'%20result='effect1_dropShadow_50_1357'/%3e%3cfeBlend%20mode='normal'%20in='SourceGraphic'%20in2='effect1_dropShadow_50_1357'%20result='shape'/%3e%3c/filter%3e%3cclipPath%20id='clip0_50_1357'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3c/clipPath%3e%3c/defs%3e%3c/svg%3e)
'%3e%3cg%20clip-path='url(%23clip0_50_1362)'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='%2318181B'/%3e%3crect%20width='39.9999'%20height='25.641'%20transform='translate(1.5%20-0.0704956)'%20fill='white'/%3e%3cpath%20d='M12.0396%208.20696C11.6901%208.62049%2011.1309%208.94666%2010.5718%208.90006C10.5019%208.34092%2010.7757%207.74683%2011.096%207.37989C11.4455%206.95471%2012.057%206.65184%2012.5521%206.62854C12.6103%207.21098%2012.3832%207.78178%2012.0396%208.20696ZM12.5463%209.01073C11.7367%208.96413%2011.0436%209.47086%2010.6592%209.47086C10.2689%209.47086%209.68066%209.03403%209.03997%209.04568C8.20708%209.05732%207.43243%209.5291%207.00725%2010.2805C6.13359%2011.7832%206.7801%2014.0081%207.62464%2015.2312C8.03817%2015.837%208.53325%2016.5009%209.18558%2016.4776C9.80297%2016.4543%2010.0476%2016.0758%2010.7931%2016.0758C11.5445%2016.0758%2011.76%2016.4776%2012.4123%2016.466C13.0879%2016.4543%2013.5131%2015.8602%2013.9267%2015.2545C14.3984%2014.5672%2014.5906%2013.8974%2014.6023%2013.8625C14.5906%2013.8508%2013.2976%2013.3557%2013.286%2011.8647C13.2743%2010.6183%2014.3053%2010.0242%2014.3518%209.98923C13.7694%209.12722%2012.8608%209.03403%2012.5463%209.01073ZM17.2233%207.32165V16.4019H18.6328V13.2975H20.584C22.3663%2013.2975%2023.6185%2012.0744%2023.6185%2010.3038C23.6185%208.53313%2022.3896%207.32165%2020.6306%207.32165H17.2233ZM18.6328%208.50983H20.2578C21.4809%208.50983%2022.1799%209.16216%2022.1799%2010.3096C22.1799%2011.457%2021.4809%2012.1151%2020.252%2012.1151H18.6328V8.50983ZM26.1929%2016.4718C27.0782%2016.4718%2027.8995%2016.0233%2028.2722%2015.3128H28.3013V16.4019H29.606V11.8822C29.606%2010.5717%2028.5576%209.72713%2026.9442%209.72713C25.4474%209.72713%2024.3407%2010.5833%2024.3%2011.7599H25.5697C25.6745%2011.2007%2026.1929%2010.8338%2026.9035%2010.8338C27.7655%2010.8338%2028.2489%2011.2357%2028.2489%2011.9754V12.4763L26.4899%2012.5811C24.8533%2012.6801%2023.968%2013.3499%2023.968%2014.5148C23.968%2015.6913%2024.8824%2016.4718%2026.1929%2016.4718ZM26.5715%2015.3943C25.8201%2015.3943%2025.3425%2015.0332%2025.3425%2014.4799C25.3425%2013.9091%2025.8027%2013.5771%2026.6821%2013.5247L28.2489%2013.4256V13.9382C28.2489%2014.7886%2027.5267%2015.3943%2026.5715%2015.3943ZM31.3475%2018.8715C32.7221%2018.8715%2033.3686%2018.3473%2033.9336%2016.7572L36.4089%209.8145H34.9761L33.3162%2015.1788H33.287L31.6271%209.8145H30.1535L32.5415%2016.4252L32.4134%2016.8271C32.1979%2017.5086%2031.8484%2017.7707%2031.2252%2017.7707C31.1145%2017.7707%2030.899%2017.759%2030.8117%2017.7474V18.8365C30.8932%2018.8598%2031.2427%2018.8715%2031.3475%2018.8715Z'%20fill='black'/%3e%3c/g%3e%3crect%20x='2'%20y='1.25'%20width='39'%20height='23'%20rx='5.5'%20stroke='%2309090B'%20stroke-opacity='0.1'/%3e%3c/g%3e%3cdefs%3e%3cfilter%20id='filter0_d_50_1362'%20x='0'%20y='0'%20width='43'%20height='27'%20filterUnits='userSpaceOnUse'%20color-interpolation-filters='sRGB'%3e%3cfeFlood%20flood-opacity='0'%20result='BackgroundImageFix'/%3e%3cfeColorMatrix%20in='SourceAlpha'%20type='matrix'%20values='0%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%20127%200'%20result='hardAlpha'/%3e%3cfeOffset%20dy='0.75'/%3e%3cfeGaussianBlur%20stdDeviation='0.75'/%3e%3cfeComposite%20in2='hardAlpha'%20operator='out'/%3e%3cfeColorMatrix%20type='matrix'%20values='0%200%200%200%200.894118%200%200%200%200%200.894118%200%200%200%200%200.905882%200%200%200%200.5%200'/%3e%3cfeBlend%20mode='normal'%20in2='BackgroundImageFix'%20result='effect1_dropShadow_50_1362'/%3e%3cfeBlend%20mode='normal'%20in='SourceGraphic'%20in2='effect1_dropShadow_50_1362'%20result='shape'/%3e%3c/filter%3e%3cclipPath%20id='clip0_50_1362'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3c/clipPath%3e%3c/defs%3e%3c/svg%3e)
'%3e%3cg%20clip-path='url(%23clip0_50_1366)'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3cg%20clip-path='url(%23clip1_50_1366)'%3e%3cpath%20d='M1.5%200.75H41.5V24.75H1.5V0.75Z'%20fill='%23FEB4C7'/%3e%3cpath%20d='M8.1902%2016.224H6.7002V9.54999H8.1902V16.224ZM11.9098%209.54999H10.4522C10.4522%2010.778%209.903%2011.9056%208.9454%2012.6432L8.3678%2013.0876L10.6054%2016.2244H12.445L10.3862%2013.338C11.3622%2012.3392%2011.9098%2010.9948%2011.9098%209.54999ZM14.2862%2016.222H12.879V9.55159H14.2862V16.222ZM18.5374%2011.6076V11.9028C18.1476%2011.6278%2017.6824%2011.4801%2017.2054%2011.48C15.8974%2011.48%2014.8366%2012.5704%2014.8366%2013.9152C14.8366%2015.26%2015.897%2016.35%2017.205%2016.35C17.682%2016.3498%2018.1472%2016.2021%2018.537%2015.9272V16.2224H19.881V11.6076H18.5374ZM18.5334%2013.9152C18.5334%2014.5708%2017.9878%2015.1024%2017.3154%2015.1024C16.643%2015.1024%2016.0978%2014.5708%2016.0978%2013.9152C16.0978%2013.2596%2016.643%2012.728%2017.3154%2012.728C17.9878%2012.728%2018.5334%2013.2592%2018.5334%2013.9152ZM32.715%2011.9028V11.6076H34.059V16.2224H32.715V15.9272C32.3252%2016.2021%2031.86%2016.3498%2031.383%2016.35C30.075%2016.35%2029.0142%2015.26%2029.0142%2013.9152C29.0142%2012.5704%2030.0746%2011.48%2031.383%2011.48C31.877%2011.48%2032.335%2011.6368%2032.715%2011.9028ZM31.493%2015.1024C32.1658%2015.1024%2032.711%2014.5708%2032.711%2013.9152C32.711%2013.2596%2032.1658%2012.728%2031.493%2012.728C30.8202%2012.728%2030.2754%2013.2592%2030.2754%2013.9152C30.2754%2014.5712%2030.8206%2015.1024%2031.493%2015.1024ZM26.6262%2011.4836C26.0894%2011.4836%2025.5814%2011.6548%2025.2418%2012.1276V11.6076H23.9038V16.2224H25.2582V13.7972C25.2582%2013.0956%2025.7158%2012.752%2026.267%2012.752C26.8578%2012.752%2027.197%2013.1148%2027.197%2013.788V16.2224H28.5394V13.2876C28.5394%2012.214%2027.709%2011.4836%2026.6262%2011.4836ZM21.9602%2011.6076H20.5842V16.2224H21.963V14.0676C21.963%2013.3408%2022.7294%2012.95%2023.2614%2012.95L23.2774%2012.9508V11.608C22.7314%2011.608%2022.2294%2011.848%2021.9602%2012.2088V11.6076ZM34.6422%2015.4524C34.6422%2014.9736%2035.0198%2014.5856%2035.4854%2014.5856C35.951%2014.5856%2036.3286%2014.9736%2036.3286%2015.4524C36.3286%2015.9312%2035.951%2016.3196%2035.4854%2016.3196C35.0198%2016.3196%2034.6422%2015.9316%2034.6422%2015.4524Z'%20fill='%2317120F'/%3e%3c/g%3e%3c/g%3e%3crect%20x='2'%20y='1.25'%20width='39'%20height='23'%20rx='5.5'%20stroke='%2309090B'%20stroke-opacity='0.1'/%3e%3c/g%3e%3cdefs%3e%3cfilter%20id='filter0_d_50_1366'%20x='0'%20y='0'%20width='43'%20height='27'%20filterUnits='userSpaceOnUse'%20color-interpolation-filters='sRGB'%3e%3cfeFlood%20flood-opacity='0'%20result='BackgroundImageFix'/%3e%3cfeColorMatrix%20in='SourceAlpha'%20type='matrix'%20values='0%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%200%20127%200'%20result='hardAlpha'/%3e%3cfeOffset%20dy='0.75'/%3e%3cfeGaussianBlur%20stdDeviation='0.75'/%3e%3cfeComposite%20in2='hardAlpha'%20operator='out'/%3e%3cfeColorMatrix%20type='matrix'%20values='0%200%200%200%200.894118%200%200%200%200%200.894118%200%200%200%200%200.905882%200%200%200%200.5%200'/%3e%3cfeBlend%20mode='normal'%20in2='BackgroundImageFix'%20result='effect1_dropShadow_50_1366'/%3e%3cfeBlend%20mode='normal'%20in='SourceGraphic'%20in2='effect1_dropShadow_50_1366'%20result='shape'/%3e%3c/filter%3e%3cclipPath%20id='clip0_50_1366'%3e%3crect%20x='1.5'%20y='0.75'%20width='40'%20height='24'%20rx='6'%20fill='white'/%3e%3c/clipPath%3e%3cclipPath%20id='clip1_50_1366'%3e%3crect%20width='40'%20height='24'%20fill='white'%20transform='translate(1.5%200.75)'/%3e%3c/clipPath%3e%3c/defs%3e%3c/svg%3e)
Detect early
Detect early signs of 1,000+ conditions
Simple and convenient
Book your test at over 2,000+ locations
Personalized plan
Actionable steps you can follow
You may also like


Become a Superpower Member
- Test for over 1,000+ conditions with our premium lab testing
- Exclusive members pricing for our marketplace
- Personalized Action Plan based on your test results
- A 24/7 clinical concierge team to answer your questions
- An AI health partner that is trained on your data